ARTIGOS
“Touchpoints”: parents and nurses’ perceptions and
satisfaction
Hélia Soares I; Sandra Martins PereiraII; Maria Céu Barbieri-FigueiredoIII
I Centro de Saúde de Angra do
Heroísmo - Unidade de Saúde da Ilha Terceira hmsoares@outlook.com
II
Instituto de Bioética - Universidade Católica Portuguesa martinspereira.sandra@gmail.com
III
Núcleo de Investigação em Enfermagem da Família / Unidade de Investigação -
Escola Superior de Enfermagem do Porto ceu@esenf.pt
Abstract Support provided to families experiencing parenting should be based on a trust relationship between nurses and parents. Satisfaction experienced with the process of care, both by parents and nurses, assumes great relevance
and can be considered as an outcome of nursing care. Purpose: To understand the
experience and meaning given by parents and nurses of participating in the
implementation of an innovative nursing intervention, with Touchpoints (TP)
methodology, of parents of children, from 11 to 24 months, and of nurses. Study
Design and Methods: Qualitative study using a phenomenological approach. Data
collection was performed using (i) field-notes (FN) written by the nurses who
implemented the TP methodology and (ii) focus groups (FG) with 10 parents of
children from the intervention group. Results: Parents considered that the TP
sessions implemented by nurses contributed to: Acquisition of knowledge and
skills; Validation of parental practices; Improvement of child behavior;
Parental confidence; Interpersonal relationship; Professional competences;
Specific competences; Satisfaction. Participant nurses perceived that the TP
methodology contributed to: Mobilization and application of TP principles;
Learning process; Parents’ interest; Feelings/emotions; Satisfaction. Clinical
Implications: Nurses caring for families should implement innovative methodologies
that facilitate adaptation to parenting, such as Touchpoints. Implementing the
TP methodology contributed to parents’ and nurses’ satisfaction. Key words: Parenting;
patient satisfaction; job satisfaction; Touchpoints methodology; nursing
intervention. Resumo O apoio prestado às famílias que vivenciam a parentalidade deve basear-se numa relação de confiança entre enfermeiros e pais. A satisfação dos clientes e dos enfermeiros durante a prestação de cuidados assume grande relevância e pode ser considerada um ganho em saúde. Objetivo: Compreender a experiência e o significado atribuído pelos pais de crianças entre os 11 e os 24 meses e dos enfermeiros que participaram na implementação da metodologia Touchpoints (TP), uma intervenção de enfermagem inovadora. Desenho do Estudo e Métodos: Estudo qualitativo de cariz fenomenológico. A recolha de dados foi efetuada através de (i) diários de itinerância dos enfermeiros que participaram na implementação da metodologia TP e da (ii) técnica de grupos focais realizada junto de 10 pais de crianças do grupo de intervenção. Resultados: os pais consideraram que as sessões TP, implementadas pelos enfermeiros, contribuíram para: Aquisição de conhecimentos e competências; Validação de práticas parentais; Melhoria do comportamento da criança; Confiança parental; Relacionamento interpessoal; Competências profissionais; Competências específicas; Satisfação. Os enfermeiros que participaram no estudo consideraram que a metodologia TP contribuiu para: Mobilização e aplicação dos princípios TP; Processo de aprendizagem; Interesse dos pais; Sentimentos/emoções; Satisfação. Implicações Clínicas: Os enfermeiros que cuidam de famílias devem implementar metodologias inovadoras que facilitem a adaptação à parentalidade, como os Touchpoints. A implementação da metodologia TP contribuiu para a satisfação dos pais e enfermeiros. Palavras-chave: Parentalidade; satisfação do cliente; satisfação profissional; metodologia “Touchpoints”; Cuidados de enfermagem.
Résumé Le soutien aux familles qui vivent la parentalité devrait
être basé sur une relation de confiance entre les infirmières et les parents.
La satisfaction vécue avec le processus de soins, par les parents et les
infirmières, revêt une grande importance et peut être considéré comme un
résultat des soins infirmiers. Objectif: comprendre l'expérience et signifiant,
de participer à la mise en œuvre d'une intervention de soins innovatrice, avec
la méthodologie Touchpoints (TP), avec des infirmières et des parents d'enfants
de 11 à 24 mois. Conception de l'étude et méthodes: étude qualitative utilisant
une approche phénoménologique. La collecte des données a été réalisée grâce à
(i) les notes de terrain des infirmières qui ont participé à la mise en œuvre
de la méthodologie TP et (ii) des groupes de discussion technique menées avec
10 parents d'enfants dans le groupe d'intervention. Résultats: Les parents
estimaient que les séances de TP, mises en œuvre par les infirmières, ont
contribué à: Acquisition de connaissances et de compétences; Validation des
pratiques parentales; Amélioration du comportement de l'enfant; La confiance
parentale; Relation interpersonnelle; Compétences professionnelles; Des
compétences spécifiques; La satisfaction. Les infirmières qui ont participé à
l'étude considère que la méthodologie de TP a contribué à: Mobilisation et
application des principes de TP; Processus d'apprentissage; L'intérêt des
parents; Sentiments / émotions; La satisfaction. Implications cliniques: Les
infirmières qui soignent les familles devraient mettre en œuvre des
méthodologies innovatrices qui facilitent l'adaptation à la parentalité, comme
Touchpoints. La mise en œuvre de la méthodologie TP a contribué à la
satisfaction des parents et des infirmières. Mots Clés:
Parenthood; satisfaction du client; satisfaction professionnelle; méthodologie
"Touchpoints"; Les soins infirmiers..
INTRODUCTION
The investment and attention given to the child at an early age is essential to
promote child health and development. This is a major concern of national and
international institutions as the World Health Organization (WHO, 2013).
Touchpoints (TP) are expected periods preceding the motor, cognitive or emotional child development. These periods can cause predictable disruption in family relationships. The development affects the child and caregivers simultaneously and it is characterized by periods of change that imply adaptation (from child and family). This can cause disorganization within the family system and relationships. Healthcare professionals can help the family to experience and cope with these periods, facilitating the adaptation/transition process.
From the perspective of a developmental model, child development within the family context is considered as a discontinuous process, in which predictable regressions encourage touchpoints to happen. This occurs because the simultaneous acquisition of skills in different areas may cause regressions in others, thus resulting in disruption of routines, feelings and familiar interactive behaviors (Brazelton & Sparrow, 2006).
The TP approach is a preventive intervention methodology that aims at (i) supporting the parent-child relationship, (ii) increasing parenting skills and (iii) strengthening the relations between the family and the baby. This approach is expected to improve child development, healthy functional families, and competent and healthy professionals (Brazelton & Sparrow, 2006).
Touchpoints methodology allows parents to identify, rationalize and anticipate the child’s behavior, recognizing the transitional moments in the emotional development and child behavior. Evidence shows that TP methodology contributes to the promotion of parenting skills, increasing self-esteem, confidence and parental power, allowing parents to respond assertive and contingently to the child’s needs, assuming an active role in his/her development (Stadtler, Brandt, Novak, & Beauchesne, 2013). This methodology allows professionals to act preventively, strengthening and facilitating their relationship with the parents (Percy, 2006). Moreover, it decreases the risk of professional burnout and increases vitality and motivation (Stadtler et al., 2013).
Touchpoints methodology includes 8 guiding principles (Table 1). Promoting children’s health and parental competences is of foremost relevance and anticipatory care is paramount (Brazelton & Sparrow, 2006; Portugal, 2013). The succession of touchpoints in a child development is like a map that can be identified and anticipated by both parents and care providers. They are much more focused on care provision of topics of interest to parents (eg., food, discipline) than in traditional milestones (e.g., crawling, walking). Negotiations with the child in connection with these touchpoints can be seen as a source of satisfaction and encouragement for the family system. Prior knowledge of these touchpoints and strategies to cope with them can help parents by reducing the negative interaction that otherwise could harm the course of child development and result in problems in different areas (e.g., sleep, food and toilet training) (Brazelton & Greenspan, 2005; Brazelton & Sparrow, 2006). Besides assuming a developmental model, Touchpoints methodology is grounded in a relational model and therefore associated to establishment of interpersonal relationships. The latter is a central concept in nursing care (Portugal, 2015) that facilitates the identification of children and parents’ needs, care planning and the implementation of interventions.
Table 1 – Touchpoints principles (adapted from Brazelton & Sparrow, 2006)
|
Principles |
Description |
|
- Recognize what you bring to the interaction |
Professional influence and is influenced by the families, his behaviors and emotions elicit his reactions and feelings. He should develop a “third ear” that helps him to develop self-reflection and maturity. |
|
- Look for opportunities to support mastery |
Professional highlights parent’s competence and self-esteem for example through observations of the child development progress and parental skills. |
|
- Use the behavior of the child as your language |
Child brings together the professional and the parents and both can see what the child’s does. His behavior is the means by which they work together and tells to the professional where he must go next. |
|
- Value disorganization and vulnerability as an opportunity |
Development is characterized by periods of normal disorganization that affect other infant systems and, simultaneously, family system. The professional use this opportunity to help parents to understand that disorganization means an anticipation of infant development progression. |
|
- Value and understand the relationship between you and the parent |
Professional enters to the family system so, he must reflect about what he represents to the family, how is distributed the power in the relationship, the professional is only an expert or also a partner? |
|
- Be willing to discuss matters that go beyond your traditional role |
Professional needs to open up their experience as a human being in relation to the families he works with to be truly effective in supporting a family’s overall well-being |
|
- Focus on the parent-child relationship |
The baby’s demands elicit expectations and responses from parents based on their own infancy and present relationships experiences. So, observe and understanding the relationship and interaction between parent and child is one of the best tools to work with the family. |
|
- Value passion wherever you find it
|
The passion of parents for children is energy, both, negative and positive that moves in the parenting process with all its challenges and joys inherent in creating and caring for a child. Therefore, the professional must find that passion and facilitate falling in love between parents and children. |
Family-centered care is essential to create a true partnership of care between health professional/patient (Jolley & Shilds, 2009). Combined with the TP methodology, it contributes to the effectiveness and quality of children and family care and (Stadtler et al., 2013). Patients’ perception of satisfaction is an indicator of quality care (Yagil, Luria, Admi, Moshe-Eilon, & Linn, 2010; Pinto, & Silva, 2013) and is influenced by the personal background and previous experiences related to healthcare, emotional support (Yagil et al., 2010; Liu, Avant, Aungsuroch, Zhang, & Jiang, 2014), health information (Eriksson & Svedlund, 2007), decision control (Campos & Graveto, 2009), technical and professional competences (Liu & Wang 2007).
Although nurses’ satisfaction is associated to patient satisfaction, it is also influenced by autonomy and involvement in clinical decision making (Campos & Graveto, 2009), quality of nursing care (Tourangeau, McGillis Hall, Doran, & Petch, 2006), “personal and professional achievement” and “organizational performance and professional/patient relationship” (Castro et al., 2011).
Despite the important role nurses have in infant and young people health, little is known about the implementation of TP methodology by nurses, even less in outermost regions frequently prevented from participating in research projects. Therefore, this study aims to understand the experience and meaning given by parents of children at the age of 11 and of 24 months and by nurses to the experience of participating in the implementation of the TP methodology in Terceira Island, Azores, Portugal.
STUDY DESIGN AND METHODS
A qualitative study was conducted using a phenomenological approach in order to
obtain an in-depth understanding of the experience and meaning given by parents
and nurses to their participation in the implementation of a quasi-experimental
design to test the TP methodology by nurses. This type or research methodology
is particularly useful to understand the meaning people build on their life
experiences, permitting the comprehension of the “insider’s” perspective. The
objective of phenomenology is the direct investigation and description of
phenomena as consciously experienced, without theories about their causal
explanations or their objective reality.
The study was conducted by nurses trained in the TP methodology, in a Primary Care Health Center, Terceira Island, Azores, Portugal, a context where population meets specific conditions of insularity and remoteness that make this context peculiar and unique. The experimental study is described in another article (Soares, Fuertes & Santos, 2015).
A major focus was given to the views, feelings and sense of satisfaction experienced both by the participant parents and nurses.
Data collection was performed using (i) the field-notes (FN) written by the two nurses who implemented the TP methodology and (ii) transcripts of focus groups (FG) recordings with the parents who were part of the intervention group (Table 2). Two diverse instruments were used for data collection (FN and FG) to adjust the best strategy for each group of participants (nurses and parents, respectively). As the number of nurses who participated in the intervention was only two, FN were more suitable than FG. Furthermore, FN are widely used in the implementation of innovative approaches aimed at changing current practices. This type of instruments allows the regular monitoring and self-assessment of experiences, feelings, and self-awareness about the development of knowledge through the intervention (Coutinho, 2011), The FN were essentially reflective, showing the experience that the two nurses lived in each TP session with the participant parents and children. The FG allowed us to gather several perspectives on the same situation as the participants were able to share the meanings attributed to the experience of participating in the implementation of the TP methodology. The two FG were conducted with 10 parents of 8 children that were part of the intervention group. Participant parents and children were recruited considering the following inclusion criteria: being healthy and clinically normal, with no sensory or motor neuron disabilities, serious illness or congenital anomalies. All parents were healthy, with no mental problems or known drug or alcohol addiction. Two fathers participated in this study. Table 2 illustrates the characteristics of the participants.
Table 2 – Sociodemographic data of the participants and technical data collection.
|
|
|
Parents n= 10 |
|
Nurses n= 2 |
|
|
|
n |
|
n |
|
Gender |
Male |
2 |
|
0 |
|
Female |
8 |
|
2 |
|
|
Age |
27-32 |
3 |
|
0 |
|
33-38 |
5 |
|
1 |
|
|
39-44 |
1 |
|
1 |
|
|
45-50 |
1 |
|
0 |
|
|
Years of formal education |
1-4 |
1 |
|
0 |
|
5-9 |
1 |
|
0 |
|
|
10-14 |
2 |
|
0 |
|
|
15-19 |
6 |
|
2 |
|
|
Technical data collection |
|
Focus groups |
|
Field-notes |
Theoretical saturation was reached after conducting 2 FG, each one with 5 parents, including a total of 10 participants.
FN were written by the two participant nurses during the implementation of TP methodology (from March 2012 to August 2013). The two FG took place in August 2013, each one lasting for about 60 minutes; the FG sessions were audio-recorded and transcribed verbatim.
The full content of the transcripts of the FG sessions and the complete FN of both participant nurses were analyzed inductively. A combination of both narrative and thematic analysis was used.
Ethical approval was obtained from the director of the primary healthcare institution where it was conducted. Furthermore, the two nurses and the parents gave their written consent in participating in the implementation program of the TP methodology and inherent data collection (FG). Results are presented anonymously with full respect for confidentiality of all participants.
RESULTS
AND DISCUSSION
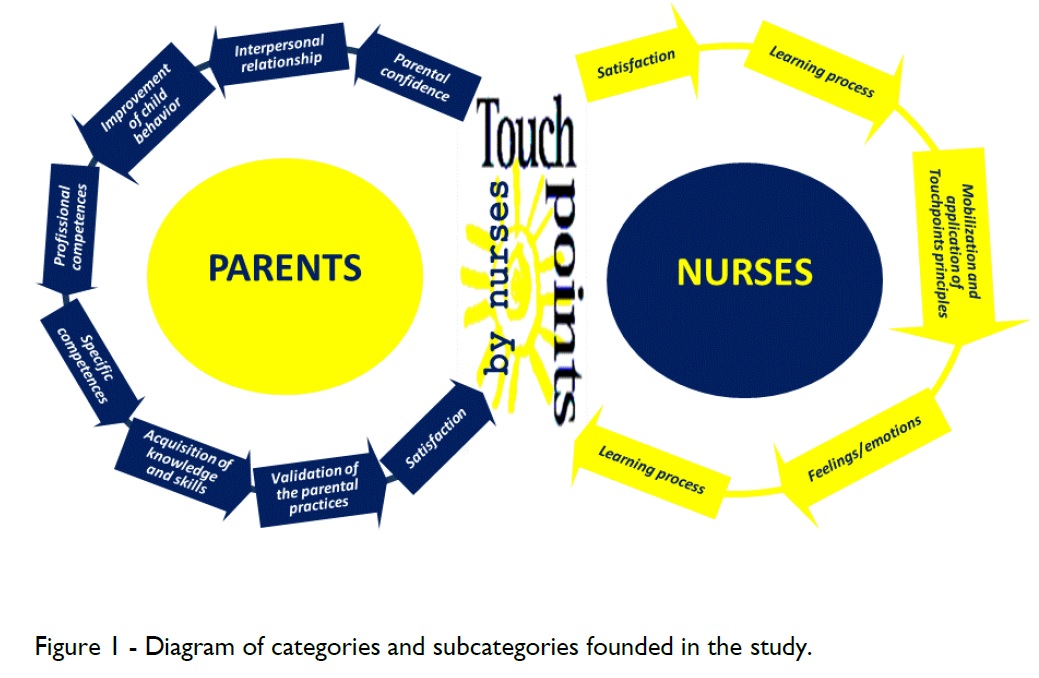
Parents who participated in the study acknowledged that the TP sessions implemented by
the nurses contributed considerably to the development of the following 8
aspects: Acquisition of knowledge and skills; Validation of parental practices;
Improvement of child behavior; Parental confidence; Interpersonal relationship;
Professional competences; Specific competences; Satisfaction.
The two nurses who implemented the abovementioned TP methodology perceived their experience as follows: Mobilization and application of TP principles; Learning process; Parents’ interest; Feelings/emotions; Satisfaction.
These concepts will be defined and further discussed as follows.
Figure 1 illustrates the perceptions of both the participant parents and nurses.
Figura 1- Diagram of categories and subcategories founded in the study
Experience of parents during the implementation of the touchpoints approach
Participant parents considered that the implementation of the TP methodology by nurses contributed mostly to their “acquisition of knowledge and skills”, namely in terms of the following aspects: the development of their child, ways to stimulate his/her development, strategies to deal with tantrums, toilet training, importance of the educational process, discipline and love in the exercise of parenting, and the opportunity to make questions. This facilitated the learning of parental role and, consequently, a better exercise and experience of parenting.
“Using those techniques that the nurse taught me, made me able to know my daughter better and this was a way to see her development clearly or to correct what she was doing wrong.” (P8); “Thereafter I tried to teach him more, see what he's doing… there were things I never paid attention to my other children; now I'm more attentive and help him to learn new things” (P2); “we had a teaching session that pleased us and functioned very well, which is how to deal with the tantrum” (P5); “start going to the potty (referring to the sphincter training) was also something that we talked about (...) I was very distracted(P6); “we explain to him what is wrong to see if he understands” (P5); “the ‘no’ is essential, ‘no’ exists and should be a persistent ‘no’ (…) if ‘no’ becomes ‘yes’ easily, doesn’t make sense” (P7); “Give lots of love, it is with love we should educate, changed deeply our approach” (P4); “there were things I had doubts and I could clarify” (P7).
Being parenting a transition process, those who experience it can be more vulnerable to risk (e.g., vulnerability to stress, illness, insufficient parenting role) (Meleis, 2011). Moreover, this transition is distinguished from others because it is a changing process that requires the acquisition of new competences, continuous learning and adaptation to the child’s development. Understanding the child’s behavior, knowing and promoting his/her development through adequate stimulation is a parents’ need and interferes with the quality of the interaction between the dyad parents-child (Bryanton, Gagnon, Hatem, & Johnston 2009). Therefore, nurses need to be aware of the family’s needs and find strategies to prepare and help parents to feel competent, secure and satisfied in the exercise of the parental role. This contributes to the well-being of the family and the promotion of child development and health.
In the parents’ speech, participating in the TP sessions contributed to the “improvement of child behavior” and was an opportunity to validate the “parental practices”, increasing “parental confidence”.
“It was spectacular and helped us a lot, dealing with his tantrums, it decreased very much (...) was excellent” (P4); “always helps, or, if only, confirms something we already were doing and was correct. Often, we do instinctively what we think best for them” (P6); “to hear and talk about important things (referring to TP sessions) made me go home and reflect, also think: ‘maybe I'm not doing wrong or I have to change it’ ” (P7).
The improvement of child behavior as a result of using the TP methodology was shown elsewhere (Brandt et al., 2010). Parents’ confidence is related to the perception of self-efficacy, investment and performance of the role (Grossklaus & Marvicsin, 2014), thus resulting in parental satisfaction and in the quality of the interaction with the child. The purpose of the TP methodology is to act preventively in order to increase the capacities of parents and their self-esteem. This increases their confidence to deal with the challenges that arise in the different stages of child development (Brazelton & Sparrow, 2006). Moreover, professionals using this methodology emphasize a positive and supportive approach focusing their intervention on the strengths and potentials of the parents.
In our study, parents felt that the nurses who applied the TP methodology presented “specific competences” at personal, relational and communicational levels..
“I valued the fact that the sessions were held by someone expert in child health (...) the sessions were more specific, more personalized, the nurse X proved to be very competent in what she does” (P6); “The nurse X has that ability to (...) is an excellent person, health services needs people like her, with feelings and attentive to patients. I think anyone caring by her will be lucky because it is a very human person, with a vocation to be a great nurse (...) is one of the best nurses I have ever met(P7); “I think that nurse X is an excellent person (...) making people feel free to speak of their problems, making diagnoses, with a power of extreme observation, knowing intervene in certain situations with the appropriate comments” (P6); “I liked very much the way the nurse spoke to my son, the way she asked things.” (P2).).
Touchpoints methodology is grounded on developmental and relational models (Brazelton & Sparrow, 2006). Holding a higher sphere of child development in its various dimensions allows the professional who uses this type of approach to help parents in identifying, streamlining and anticipating child behavior, improving their understanding about the transitory moments of the child’s emotional behavior. According to Lopes, Catarino and Dixe (2010), nurses not only need specialized knowledge about child development and health but also on methodologies that allow an interactive and positive relationship with parents. This specialized knowledge gives security to parents (Oommen, Rantanen, Kaunonen, Tarkka, & Salonen, 2011). In addition to enabling professionals to obtain an appropriate response to parents’ needs, parents emphasized the way this knowledge was shared through personal and professional skills. Participant parents highlighted the passion transmitted by the nurses in the way they acted and lived their profession, which distinguished them from other nurses making them look “specials”.
The communication competences and interactive capacities expressed by nurses in their daily practice are not only associated with their personal characteristics. These attributes also emerge from the relational paradigm that underlies the TP model (Brazelton & Sparrow, 2006), promoting and facilitating the alliance and trustful relationship with parents. It is interesting to notice that the theme “interpersonal relationship” was one of the themes with the highest number of categories, thus showing the considerable appreciation parents gave to this dimension of nursing care during TP sessions. This theme is subdivided into eight sub-themes: “Observation attentive/affection”; “Person-centered care/approach”; “Presence”; “Friendship”; “Trust”; “Tranquility”; “Dedication”; “Support”..
“Most of the opinions we have are statements that people give and give a hundred kids; what I noticed here was that the nurse tried to give appropriate advice to our son in particular in an adapted way according to our way of dealing with life, our extract, our profession. She could adapt the advice to our son specifically and to us and this is something that is really rare because most people give hints” (P4); “In addition, we also have a friend (referring to the nurse who held sessions)” (P8); “We also noticed, at that moment, (…) the nurse X, was available and attentive to us and to our child, reading what was in front, I noticed.” (P6); “ the nurse X had a very different purpose, she devoted herself to us, to that child” (P6); “there were things that the nurse X noted in my son that even paying to a pediatrician I never saw. She played with him, watched, evaluated the development and saw what he was able to do, at the same time managing to be affectionate” (P7); “nurse X was there to answer and say exactly what was right, we would not have to ask someone else, you know that she would say exactly what should be” (P8); “that support is very important” (P4); “that nurse transmit a peace and I felt this when we met...” (P2).).
The concept of interpersonal relationship is central in nursing care (Portugal, 2015) and it is influenced by communicational competences (Yagil et al., 2010; Kinder & Allen, 2014). As in the Family Centered Care philosophy (Kuo et al., 2012), TP methodology focuses on partnership, support and collaboration with parents and on the assumption that they are “the experts” in their child knowledge (Brazelton & Sparrow, 2006).
The accessibility and proximity with nurses interferes directly in the quality of the interaction with the family (Lopes, Catarino, & Dixe, 2010). In addition, nurses’ availability affects the parents’ satisfaction toward nursing care (Magnusson, Lagerberg, & Sundelin, 2012).
The patients’ trust in healthcare professionals contributes to a greater demand for care, adherence to treatment and continuity of care determining the satisfaction with the care provided (Thom et al., 2014).
In our study, parents considered that the TP sessions contributed to their “Satisfaction”.
“The sessions were very beneficial for everyone, it makes a big difference” (P6); “I loved it, if it were possible I'd like to continue these sessions” (P9
Parents’ satisfaction with healthcare and parenting is crucial in the development of parental competences and abilities to care for their child (Grossklaus & Marvicsin, 2014). Moreover, this satisfaction is an indicator of a health gain and care outcome. These findings are aligned with another study (Soares, et al., 2015) suggesting that the TP methodology, in this population, was associated to high levels of parents’ satisfaction. Table 3 presents the summary of the themes and subthemes of the dimension “Experience of parents during the implementation of the Touchpoints approach”.
Table 3 - Summary of themes, subthemes and dimension: Experience of parents and nurses during the implementation of the Touchpoints approach
|
DIMENSION |
Theme |
Subtheme |
|
EXPERIENCE OF PARENTS DURING THE IMPLEMENTATION OF THE TOUCHPOINTS APPROACH
|
Acquisition of knowledge and skills |
Knowing the development of the child |
|
Tantrums |
||
|
Educational process |
||
|
Love / affection |
||
|
Clarify doubts |
||
|
Discipline |
||
|
Development stimulation |
||
|
Toilet training |
||
|
Interpersonal relationship |
Attentive observation and affection |
|
|
Person-centered care/approach |
||
|
Presence |
||
|
Friendship |
||
|
Trust |
||
|
Tranquility |
||
|
Dedication |
||
|
Support |
||
|
Parental confidence |
|
|
|
Improvement of child behavior |
|
|
|
Professional competences |
|
|
|
Validation of the parental practices |
|
|
|
Specific competences |
Personal competences |
|
|
Relational competences |
||
|
Communicational competences |
||
|
Satisfaction |
|
|
|
EXPERIENCE OF NURSES DURING THE IMPLEMENTATION OF THE TOUCHPOINTS APPROACH |
Mobilization and application of Touchpoints principles |
Recognize what you bring to the interaction |
|
Look for opportunities to support mastery |
||
|
Use the behavior of the child as your language |
||
|
Value disorganization and vulnerability as an opportunity |
||
|
Value and understand the relationship between you and the parent |
||
|
Be willing to discuss matters that go beyond your traditional role |
||
|
Focus on the parent-child relationship |
||
|
Value passion wherever you find it |
||
|
Learning process |
|
|
|
Parents’ interest |
|
|
|
Negative feelings/emotions |
Anxiety |
|
|
Difficulty |
||
|
Nostology |
||
|
Discomfort |
||
|
Positive feelings/emotions |
Motivation |
|
|
Gratifying and rewarding sensation |
||
|
Satisfaction |
|
Experience of nurses during the implementation of the touchpoints approach
The participant nurses considered that the experience of participating actively in the implementation of the TP methodology allowed them to fully “Mobilize and apply the TP principles”. From the 8 TP principles the one that emerged more expressively in the FN was: “Recognize what you bring to the interaction”. This principle highlights the relevant contribution this methodology gives to personal and professional development as a result of the process of reflection and self-awareness it generates.
“Parental words do not come out from my mind. There is indeed to change behaviors, however difficult it may be. A whole relationship can be compromised with the first impact we give and receive (...) the judgments must stay outside the service.” (E2).
This is aligned with Yagil et al. (2010) who emphasized the need for nurses to develop self-knowledge. This is of foremost relevance as it helps nurses to become aware of the stereotypes they have and that may harm the relationship with patients.
According to the nurses’ own words, the implementation of TP methodology was associated with positive and negative “Feelings/emotions”.
The “positive feelings/emotions” referred to: “Motivation” and “Gratifying and rewarding sensation”.
“I felt an urge to talk to the mother, ‘playing’ with the child and be attentive to all was happening around me” (E2); “The mother expression of interest and surprise made me feel rewarding and useful, probably, I could help her (…) to interpret her daughter behavior making her feel secure, confident and knowledge empowered” (E1).
Professionals’ sense of effectiveness contributes to a higher investment of time in these tasks (e.g., vaccination, perform physical exams and health histories, provide health promotion, counseling and education) being associated to professional empowerment and to the quality of care (Hernandez-Marrero, 2006). Consequently, these professionals will have more work-related satisfaction, thus feeling rewarded, empowered and engaged (Bandura, 1997 cited by Grossklaus & Marvicsin, 2014).
Although much less expressively, the theme “negative feelings/emotions” was also found in the FN namely in terms of: “Anxiety”, “Difficulty”, “Discomfort” and “Nostalgia”..
“It is, indeed, difficult to follow the mother or both parents, the child and the whole surroundings of the moment.” (E2); “In this session I felt very upset when mom and dad said that health professionals (nurses) did not treat users equally, and if they don’t enjoy their profession shouldn’t be there, father said yet that in many nursing visits he held back for not ‘explode’”. (E2); “I’m already beginning to miss these families because I know next month is the last one I will be with children and families, it is clear that they will be in my memory, and anybody can strip it by my mind. I found that I really love and want to be with families, with the children” (E1).
Even if “Nostalgia” can be considered a negative feeling/emotion, in this particular case it may also reflect something positive associated with the bond, depth, nature and quality of the relationship nurse/family established in the interaction process with families. Indeed, it is to remember with joy and fulfillment times and experienced relationship processes, wishing to experience them again. In our view, the depth, nature and quality of the relationship developed and lived with the other and the impact and importance it had in the life of both are essential and reflects the components for the construction and development of a true therapeutic relationship
Nurses also highlighted the “learning process” associated with the implementation of TP methodology. Ingredients
“I learned a lot from all families, each with its own style, each with different skills but, all made me see there are no perfect families but all parents want the best for their children” (E1).
The conceptual framework of the TP methodology and its principles guide the professional and the relationship established with families. This triggers the professional to “open-up” to others (e.g., parents), questioning, reflecting on his/her actions and on him/herself as human being. The richness of this experience provides opportunities for learning and personal development.
“Parents’ interest” was also valued by the participant nurses.
“Parents consider information provided very pertinent and saying that should always be given, they left the room thanking the accompaniment available” (E2).
Patient interest and recognition of the quality of care is an aspect that greatly influences the motivation and gratification experienced by nurses. Although conducted in different contexts, evidence shows that the recognition by the healthcare beneficiaries contributes to feelings of fulfillment among health professionals (Pereira, Fonseca & Carvalho, 2012; Smart et al., 2014).
Finally, nurses highlighted the “Satisfaction” related with the completion of the TP sessions.
“I loved to make this assessment because Z is a child who exudes tranquility, love and good humor, demonstrates - Happiness - in the presence of parents, he feels security to explore, imitate and interact with me”. (E2).
As suggested by Stadtler et al. (2013), nurses using TP methodology in their practices feel satisfaction and this is an important outcome of this approach. Table 3 presents the summary of themes and subthemes of the dimension “Experience of nurses during the implementation of the Touchpoints approach”.
STRENGTHS
AND LIMITATIONS
As far as we know, this is the first study focusing on the implementation of TP
methodology by nurses in the outermost region of Azores. This is of relevance
as people living in this region are often excluded from relevant research,
which may increase their sense of isolation and vulnerability. Furthermore, it
relates nurses’ perceptions and satisfaction to the ones of the parents.
Nevertheless, a few limitations need to be mentioned: (i) The experiences and
meanings among parents and professionals were obtained using different
instruments (FG vs. FN); however, tools and data collection techniques had to
be adapted to specificity of environment and participants. (ii) A
mixed-methods approach could have reinforced the findings. Our findings refer
only to qualitative data and could have been complemented by the use of a
satisfaction scale for professionals and parents.
Despite these limitations, it is relevant to emphasize the novelty of the use of TP by nurse. This is also a relevant feature, which may contribute to the effective implementation of this methodology in practice, without additional costs to the healthcare system. Moreover, the combination of perspectives and techniques focusing on the experience of the participants, meaning and satisfaction, brings a better yield to this subject.
CLINICAL IMPLICATIONS
This study addresses the experience of implementing the TP methodology by nurses,
focusing on parents who are in a transition process, i.e., parenting, in the
conviction that it can be a relevant contribution to nursing practice, health
promotion and care. This can be achieved through the integration of this
methodology in practice, which requires the interaction and relational
dimension that are nuclear in nursing, contributing to the development of
parental skills through a preventive approach based on the family’s strengths.
Based on our findings we can assume that the implementation of the TP methodology in practice contributes not only to the development of parenting skills, facilitating their transition process of parenthood, but it also contributes to parental and professional emotional well-being and satisfaction.
The results of this study suggest that the use of this methodology contributes to professional and costumers’ satisfaction which can be considered a care outcome. In fact, we can assume that satisfied professionals and satisfied customers may be synonymous of high and good quality care. Therefore, based on our findings we recommend the integration of TP methodology in nursing education at undergraduate and post-graduate levels.
REFERENCES
Brandt, K. A., & Murphy, J. M. (2010). Touchpoints in a nurse home visiting program. In B. M. Lester & J. Sparrow (Eds.), Nurturing children and families: Building on the legacy of T. Berry Brazelton (pp. 177–191). Chichester, UK: Blackwell.
Brazelton, T.B., Sparrow, J.D (2006). Touchpoints: Birth to Three: Your child’s emotional and behavioral development. Cambridge, MA: Da Capo Press.
Brazelton, T, B., Greenspan S. (2005). Las necesidades básicas de la infancia. Barcelona: Graó.
Bryanton, J., Gagnon, A.J., Hatem, M., & Johnston, C. (2009). Does Perception of the Childbirth Experience Predict Women’s early parenting behaviors? Research in Nursing & Health, 32(2), 191-203. doi:10.1002/nur.20314
Campos, D., & Graveto, J. (2009). The role of nurses and patients' involvement in the clinical decision-making process. Rev Latino-Am Enfermagem, 17(6), 1065-1070. Retrieved July 14, 2015, from http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692009000600021&lng=en&tlng=en. Doi:10.1590/S0104-11692009000600021
Castro, J., Lago, H., Fornelos, M., Novo, P., Saleiro, R., Alves, O. (2011). The influence of job rotation in the job satisfaction of nurses in a surgical service. Revista portuguesa de Saúde Pública, 29(2), 157-172.
Charmaz K. (2009). Shifting the Grounds: Constructivist Grounded Theory Methods for the Twenty-first Century, in J. Morse, P. Stern, J. Corbin, B. Bowers, K. Charmaz, & A. Clarke, Developing Grounded Theory: The Second Generation, Walnut Creek, CA: Left Coast Press.
Coutinho, C. (2011). Metodologia de investigação em ciências sociais e humanas: teoria e prática. Coimbra: Almedina.
Curtis, E. & Redmond, R. (2007). Focus Groups in Nursing Research. Nurse Researcher. 14, 25–37.
Eriksson U. & Svedlund M. (2007) Struggling for confirmation – patients’ experiences of dissatisfaction with hospital care. Journal of Clinical Nursing, 16, 438–446.
Grossklaus, H., Marvicsin, D. (2014). Parenting efficacy and its relationship to the prevention of childhood obesity. Pediatric Nursing, 40(2), 69–86.
Hernandez-Marrero, P. (2006). Determinants of self-perceived managerial effectiveness in the Canarian Health System. Published doctoral dissertation. University of Toronto, Canada. ISBN 978-0494160121.
Kuo, D.Z., Houtrow, A.J., Arango, P., Kuhlthau, K.A., Simmons, J.M. & Neff, J.M. (2012). Family-centered care: current applications and future directions in pediatric health care. Maternal Child Health Journal 16(2), 297-305. doi:10.1007/s10995-011-0751-7
Kuosmanen L., Hätönen H., Jrykinen A.R., Katajisto J. & Välimäki M. (2006) Patient satisfaction with psychiatric inpatient care. Journal of Advanced Nursing, 55(6), 655–663.
Liu,Y., Avant, K., Aungsuroch, Y., Zhang, X-Y., & Jiang, P. (2014). Patient outcomes in the field of nursing: A concept analysis. International Journal of Nursing Sciences, 1(1), 69-74.doi:10.1016/j.ijnss.2014.02.006
Lopes, M., Catarino, H., & Dixe, M. (2010). Positive Parenting and Nursing: Systematic literature Review. Journal of Nursing Referência, 3(1), 109-118. doi:10.12707/RII1047
Magnusson, M., Lagerberg, D., & Sundelin, C. (2012). Organizational differences in early child health care - mothers' and nurses' experiences of the services. Scandinavian Journal Of Caring Sciences, 26(1), 161-168. doi:10.1111/j.1471-6712.2011.00910.x
Meleis, A.I. (2011). Theoretical nursing: Development and progress (5th Ed.). Philadelphia, PA: Lippincott Williams & Wilkins.
Oommen, H., Rantanen, A., Kaunonen, M., Tarkka, M., & Salonen, A. (2011). Social support provided to Finnish mothers and fathers by nursing professionals in the postnatal ward. Midwifery, 27(5), 754-761. doi:10.1016/j.midw.2010.06.017
Pereira, S., Fonseca, A. & Carvalho, A. (2012). Burnout in nurses working in Portuguese palliative care teams: a mixed methods study. International Journal of Palliative Nursing, 18(8), 373–381. doi: 10.12968/ijpn.2012.18.8.373
Pinto, S., & Silva, E. (2013). Quality and satisfaction with the emergency pediatric service: the perspective of children’s parents. Journal of Nursing Referência, 3(9), 95-103. doi:10.12707/RIII1285
Portugal(2015). Regulamento n.º 190/2015 de 23 abril - Diário da República nº 79/2015-II Série. Regulamento do Perfil de Competências do Enfermeiro de Cuidados Gerais: Ordem dos Enfermeiros
Portugal, Direção-Geral da Saúde (2013). Programa Nacional de Saúde Infantil e Juvenil. Norma nº 010/2013. Lisboa, Portugal: DGS.
Portugal. Ministério da Saúde; Direção-Geral da Saúde. (2012). Plano Nacional de Saúde 2012-2016. [Internet]. Lisboa. [cited 2015 jun. 15]. ]. Available from: http://pns.dgs.pt/pns-versao-completa
Smart, D., English, A., James, J., Wilson, M., Daratha, K. B., Childers, B., & Magera, C. (2014). Compassion fatigue and satisfaction: A cross-sectional survey among US healthcare workers. Nursing & Health Sciences, 16(1), 3-10. doi:10.1111/nhs.12068
Soares, H., Fuertes, M., & Santos, M. (2015).The impact of Touchpoints intervention on parental perception of the quality and promotion of the relationship with nurses (Under review).
Stadtler, A. C., Brandt, K. A., Novak, J. C., & Beauchesne, M. A. (2013). Reflections on T. Berry Brazelton, MD's influence on pediatric nursing. Journal of Child and Adolescent Psychiatric Nursing, 26(4), 234-238. doi:10.1111/jcap.12057
Thom, D., Hessler, D., Willard-Grace, R., Bodenheimer, T., Najmabadi, A., Araujo, C., & Chen, E. (2014). Does health coaching change patients’ trust in their primary care provider? Patient Education and Counseling, 96, 135 – 138. doi: 10.1016/j.pec.2014.03.018
Tourangeau, A., McGillis Hall, L., Doran, D., & Petch, T. (2006). Measurement of nurse job satisfaction using the McCloskey Mueller satisfaction scale. Nursing Research, 55(2), 128-136.
World Health Organization (2013). Counselling for maternal and newborn health care: A handbook for building skills. World Health Organization: Geneva. http://apps.who.int/iris/bitstream/10665/44016/1/9789241547628_eng.pdf
Yagil, D., Luria, G., Admi, H., Moshe-Eilon, Y., & Linn, S. (2010). Parents, spouses, and children of hospitalized patients: evaluation of nursing care. Journal Of Advanced Nursing, 66(8), 1793-1801. doi:10.1111/j.1365-2648.2010.05315.x
Contacto: Hélia Soares, Centro de Saúde de Angra do Heroísmo, Unidade de Saúde da Ilha Terceira, Canada dos Melancólicos, 9700-121 Angra Do Heroismo, Portugal / hmsoares@outlook.com (recebido em novembro de 2015, aceite para publicação em abril de 2016)
Sandra Martins Pereira, Instituto de Bioética,Universidade Católica Portuguesa, R. de Diogo Botelho 1327, 4169-005 Porto, Portugal / martinspereira.sandra@gmail.com
Maria Céu Barbieri-Figueiredo, Núcleo de Investigação em Enfermagem da Família/Unidade de Investigação Escola Superior de Enfermagem do Porto, Rua Dr. António Bernardino de Almeida 4200-072 Porto, Portugal / ceu@esenf.pt
{kind=link}